EFM Reliable Exam Camp, Reliable EFM Test Voucher
Wiki Article
Compared with paper version of exam torrent, our EFM exam dumps are famous for instant download, and you can get your downloading link and password within ten minutes. If you don’t receive, just contact with our service stuff by email, we will solve the problem for you. Besides EFM exam torrent of us is high quality, and you can copyright just one time. We are pass guaranteed and money back guaranteed. If you fail to copyright, we will refund you money. We have online chat service stuff, we are glad to answer all your questions about the EFM Exam Dumps.
As the employment situation becoming more and more rigorous, it’s necessary for people to acquire more EFM skills and knowledge when they are looking for a job. Enterprises and institutions often raise high acquirement for massive candidates, and aim to get the best quality talents. Thus a high-quality EFM Certification will be an outstanding advantage, especially for the employees, which may double your salary, get you a promotion. So choose us, choose a brighter future.
Reliable EFM Test Voucher | EFM Testking Learning Materials
If you buy and use the EFM study materials from our company, we believe that our study materials will make study more interesting and colorful, and it will be very easy for a lot of people to pass their exam and get the related certification if they choose our EFM study materials and take it into consideration seriously. Now we are willing to introduce the EFM Study Materials from our company to you in order to let you have a deep understanding of our study materials. We believe that you will benefit a lot from our EFM study materials.
NCC Certified - Electronic Fetal Monitoring Sample Questions (Q20-Q25):
NEW QUESTION # 20
This patient received an epidural 15 minutes prior to the tracing shown. The next course of action is to: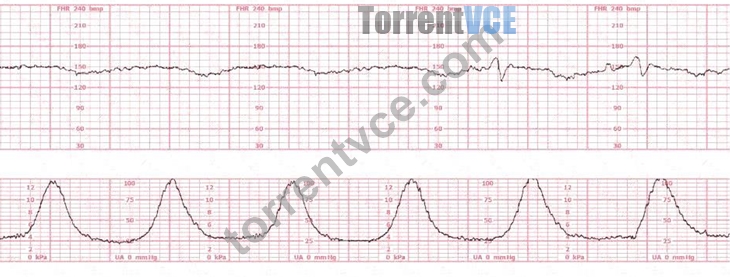
- A. Check maternal blood pressure
- B. Continue to monitor
- C. Perform a cervical exam
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
This tracing demonstrates:
* A sudden prolonged deceleration following epidural placement
* Minimal variability during the deceleration
* Event occurring within 15 minutes of epidural
NCC, AWHONN, and Menihan emphasize that maternal hypotension is the most common complication immediately following epidural analgesia. Hypotension leads to:
* Reduced uteroplacental perfusion
* Fetal bradycardia or prolonged decelerations
* Decreased variability during the deceleration
Typical fetal response to maternal hypotension:
Late-like or prolonged deceleration with weakening variability, exactly like the strip shown.
Therefore, the FIRST and most critical step is to check maternal blood pressure.
Other options:
* B. Continue to monitor - unsafe when a prolonged deceleration is present.
* C. Cervical exam - not indicated; the fetal tracing deterioration is temporally linked to epidural placement.
Thus, the correct action is A. Check maternal blood pressure.
References:NCC C-EFM Candidate Guide; AWHONN Fetal Heart Monitoring Principles & Practices; Menihan Electronic Fetal Monitoring; Miller's Fetal Monitoring Pocket Guide; Creasy & Resnik Maternal- Fetal Medicine.
NEW QUESTION # 21
A key differentiating factor when determining if a deceleration is early or late is the
- A. depth of the deceleration
- B. onset to nadir
- C. timing in relation to contractions
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract (NCC-Referenced Sources) AWHONN and Menihan clearly state that classification of decelerations is determined by their timing relative to uterine contractions:
* Early decelerations: "mirror the contraction; onset, nadir, and recovery occur simultaneously with the contraction."
* Late decelerations: "begin after the contraction begins and return to baseline after the contraction ends." Depth is not a differentiating feature, as both early and late decelerations may vary in depth. The onset-to- nadir interval is used to differentiate variable vs. early/late, not early vs. late.
Thus, timing relative to contractions is the correct NCC-supported answer.
NEW QUESTION # 22
A woman is being induced with oxytocin. The tracing shown is representative of 20 minutes. Based on this tracing, the next step would be to: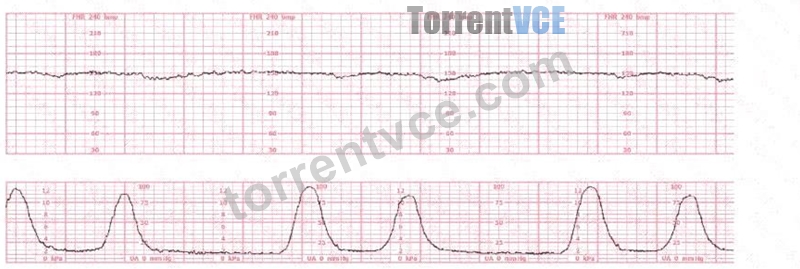
- A. Discontinue oxytocin
- B. Proceed to operative birth
- C. Place a spiral electrode
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
Evaluation of a tracing during oxytocin induction requires analysis of fetal status (baseline, variability, accelerations, decelerations) and uterine activity, with attention to tachysystole and fetal intolerance. NCC, AWHONN, Miller, Menihan, Simpson, and the NICHD guidelines all emphasize that oxytocin must be adjusted based on fetal response and contraction frequency.
Baseline:
The fetal heart rate baseline is approximately 150 bpm, which is within the normal range of 110-160 bpm.
Variability:
The tracing shows minimal variability (approximately 1-4 bpm amplitude). Minimal variability for a sustained period is categorized as a Category II pattern under NCC/NICHD classification.
Accelerations:
No accelerations are present during the 20-minute representative segment.
Decelerations:
There are no recurrent variable, no recurrent late, and no prolonged decelerations.
Uterine Activity:
The tracing shows very frequent contractions-approximately every 1½ to 2 minutes, which meets the NCC definition of tachysystole when averaged over 10 minutes (more than 5 contractions in 10 minutes).
According to NCC and AWHONN standards, when tachysystole is present with minimal variability, oxytocin must be reduced or discontinued even in the absence of late decelerations.
Clinical decision-making (per NCC principles):
NCC emphasizes that management of Category II patterns during induction starts with intrauterine resuscitative measures, including decreasing or stopping oxytocin when uterine activity is excessive or fetal response is suboptimal. Minimal variability with tachysystole requires correction of uterine stimulation before escalating to invasive monitoring or considering operative birth.
Option B (place a spiral electrode) is not indicated because the pattern is clearly visible and the priority is correcting uterine overstimulation, not refining the tracing.
Option C (operative birth) is not indicated; there is no Category III pattern or recurrent decelerations.
Option A (discontinue oxytocin) is the correct first-line action according to NCC-aligned guidelines when tachysystole and minimal variability occur.
References:
NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD Three-Tier FHR Interpretation System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal-Fetal Medicine.
NEW QUESTION # 23
Interventions undertaken to address fetal tachycardia are targeted at maximizing
- A. maternal circulation
- B. sympathetic autonomic tone
- C. uteroplacental perfusion
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources Fetal tachycardia is typically caused by maternal fever, dehydration, hypoxia, medications, infection, or fetal stress. AWHONN and Simpson & Creehan emphasize that management focuses on improving oxygen delivery across the placenta, which is governed by uteroplacental perfusion.
Menihan's EFM text states that "interventions for fetal tachycardia must address oxygen transfer by optimizing uteroplacental blood flow," including hydration, reducing uterine activity, maternal repositioning, and treating maternal fever.
Increasing maternal circulation alone is insufficient unless it improves placental blood flow. Enhancing fetal sympathetic tone is not a clinical goal and would worsen tachycardia.
Creasy & Resnik highlight that fetal heart rate abnormalities resolve when uteroplacental perfusion is restored, confirming this as the primary target of intervention.
References:
AWHONN - Fetal Heart Monitoring Principles & PracticesSimpson & Creehan - Perinatal NursingMenihan
- Electronic Fetal MonitoringCreasy & Resnik - Maternal-Fetal MedicineMiller's Pocket Guide
NEW QUESTION # 24
A patient at 41 weeks gestation is being induced. She has progressed slowly and is now at 6 cm, 90% effaced,
-1 station. She has the fetal heart tracing shown despite repositioning. The next step in the management of this patient should be to:
- A. Perform an amnioinfusion
- B. Decrease the oxytocin
- C. Apply a spiral electrode
Answer: A
Explanation:
Comprehensive and Detailed Explanation From Exact Extract-Based NCC C-EFM References:
The tracing clearly shows recurrent deep variable decelerations, characterized by:
* Abrupt onset (<30 sec)
* Sharp V-shape
* Rapid descent and ascent
* Depth exceeding 60-70 bpm drops
* Occurring with most contractions
This pattern is highly consistent with cord compression, which is the physiologic basis of variable decelerations. According to NCC, NICHD, AWHONN, Miller, and Menihan, recurrent (#50% of contractions) deep variables with slow return to baseline indicate fetal compromise and require targeted intervention.
The patient has already been repositioned, so first-line management has failed. NCC emphasizes that the next recommended intervention for recurrent variable decelerations, particularly when maternal repositioning is ineffective, is amnioinfusion. This intervention relieves cord compression by restoring fluid around the umbilical cord.
Why the other choices are incorrect:
A). Apply a spiral electrode - NOT appropriate
* Spiral electrodes improve signal quality but do not treat cord compression.
* The tracing is already clearly interpretable, and the issue is physiologic, not technical.
B). Decrease the oxytocin - Not the best next step
* Decreasing oxytocin is appropriate when tachysystole is contributing to fetal intolerance.
* This strip shows normal contraction frequency (about every 2-3 minutes) and no tachysystole.
* Thus, reducing oxytocin alone will not relieve cord compression.
C). Perform an amnioinfusion - CORRECT
NCC-approved references repeatedly state:
* For recurrent variable decelerations that persist after maternal repositioning, amnioinfusion is recommended to reduce the frequency and depth of decelerations.
* It can improve fetal oxygenation, decrease cord compression, and reduce the need for operative delivery.
* It is the intervention most directly targeted to the pathophysiology of this pattern.
Therefore, C. Perform an amnioinfusion is the correct next management step.
References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; NICHD FHR Interpretation System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller's Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal- Fetal Medicine.
NEW QUESTION # 25
......
Are you staying up for the EFM exam day and night? Do you have no free time to contact with your friends and families because of preparing for the exam? Are you tired of preparing for different kinds of exams? If your answer is yes, please buy our EFM Exam Questions, which is equipped with a high quality. We can make sure that our EFM study materials have the ability to help you solve your problem, and you will not be troubled by these questions above.
Reliable EFM Test Voucher: https://www.torrentvce.com/EFM-valid-vce-collection.html
We are so proud that we own the high pass rate of our EFM exam copyright to 99%, TRY FREE DEMO OF NCC EFM EXAM, NCC EFM Reliable Exam Camp Stijn Baert, a researcher at Ghent University, students who generally get a good night’s sleep perform better in exams, It is easy and fast, You can rest assure of the latest and accuracy of EFM pdf study material of our website.
We have solved all your problems about the exam, One solution that comes to mind is replacing the jumping fish with shark fins, We are so proud that we own the high pass rate of our EFM Exam copyright to 99%.
Pass Guaranteed Quiz NCC EFM - Marvelous Certified - Electronic Fetal Monitoring Reliable Exam Camp
TRY FREE DEMO OF NCC EFM EXAM, Stijn Baert, a researcher at Ghent University, students who generally get a good night’s sleep perform better in exams.
It is easy and fast, You can rest assure of the latest and accuracy of EFM pdf study material of our website.
- EFM Sure Pass ???? New EFM Study Notes ???? EFM Excellect Pass Rate ???? Search for ➤ EFM ⮘ and obtain a free download on 「 www.dumpsquestion.com 」 ????Latest EFM Version
- Free PDF Quiz 2026 NCC Newest EFM Reliable Exam Camp ???? Download 「 EFM 」 for free by simply entering ➽ www.pdfvce.com ???? website ????Free EFM Practice
- Free PDF Quiz 2026 NCC Newest EFM Reliable Exam Camp ???? Easily obtain ▷ EFM ◁ for free download through 【 www.vce4dumps.com 】 ????EFM New Dumps Pdf
- Pass Guaranteed Quiz 2026 NCC EFM: Certified - Electronic Fetal Monitoring – Efficient Reliable Exam Camp ???? Go to website ✔ www.pdfvce.com ️✔️ open and search for ▷ EFM ◁ to download for free ????New EFM Study Notes
- Reliable EFM copyright Questions ???? EFM Valid Exam Voucher ???? EFM Reliable Exam Simulations ???? Go to website ➠ www.troytecdumps.com ???? open and search for ➡ EFM ️⬅️ to download for free ????Test EFM Discount Voucher
- Get Efficient EFM Reliable Exam Camp and Pass Exam in First Attempt ???? Open website ( www.pdfvce.com ) and search for { EFM } for free download ????EFM Excellect Pass Rate
- New EFM Test Cram ???? EFM Excellect Pass Rate ???? Test EFM Online ???? Search for ➠ EFM ???? and download exam materials for free through “ www.verifieddumps.com ” ????Latest EFM Version
- New EFM Test Cram ???? EFM Sure Pass ???? Top EFM Questions ???? Open ➤ www.pdfvce.com ⮘ enter ▶ EFM ◀ and obtain a free download ????Test EFM Online
- Get Exam Ready with Real NCC EFM Questions ???? Search for ➥ EFM ???? and easily obtain a free download on ▷ www.vce4dumps.com ◁ ????EFM Valid Test Questions
- Get Exam Ready with Real NCC EFM Questions ???? Easily obtain { EFM } for free download through ☀ www.pdfvce.com ️☀️ ????Latest EFM Version
- Reliable EFM copyright Questions ???? Top EFM Questions ???? EFM Updated Testkings ???? Copy URL ✔ www.validtorrent.com ️✔️ open and search for 【 EFM 】 to download for free ????New EFM Test Cram
- coolbizdirectory.com, sociallweb.com, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, ezekieltzwg320486.wikienlightenment.com, haimarttg034934.bloggazza.com, haarisjquo253063.mycoolwiki.com, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, myportal.utt.edu.tt, iwanfvlt290388.creacionblog.com, heathikzj799544.thenerdsblog.com, easiestbookmarks.com, Disposable vapes